Fentanyl should be given only in an environment where the airway can be controlled and by personnel who can control the airway.
The dose of fentanyl is adjusted individually according to age, body weight, physical status, pathological condition, co-medication and as well as type of surgical procedure and type of anaesthesia.
For guidance, the following dosage schedules are proposed. For other special dosage recommendations please refer to the literature.
Neurolept analgesia and neurolept anaesthesia: For neurolept analgesia adults normally will require an initial dose of 50 to 100 micrograms (0.7-1.4 microgram/kg) fentanyl, slowly injected intravenously in combination with a neuroleptic (preferably droperidol). If necessary a second dosage of 50 to 100 micrograms (0.7-1.4 microgram/kg) fentanyl can be given 30 to 45 minutes after the initial dose.
For neurolept anaesthesia under the condition of assisted ventilation adults in general will require an initial dose of 200 to 600 micrograms (2.8-8.4 micrograms/kg) fentanyl slowly injected intravenously in combination with a neuroleptic (preferably droperidol).
The dosage depends on the duration and the severity of the surgical procedure and on the medication used for general anaesthesia. For maintenance of anaesthesia, additional doses of 50 to 100 micrograms (0.7-1.4 microgram/kg) fentanyl can be given every 30 to 45 minutes. The time intervals and doses of these additional administrations have to be adjusted according to the course of the surgical procedure.
Analgesic component in general anaesthesia: Adults: Premedication: 50 to 100 micrograms (1 to 2 mL) fentanyl administered intramuscularly 30 to 60 minutes prior to surgery (modified for high risk patients).
For induction: If fentanyl is used as an analgesic component in general anaesthesia with intubation and ventilation of the patient, in adults initial fentanyl doses of 70-600 microgram (1-8.4 microgram/kg) can be applied as adjunct to general anaesthesia.
For maintenance of analgesia during general anaesthesia, additional doses of 25-100 microgram (0.35-1.4 microgram/kg) fentanyl are to be injected subsequently. The time intervals and the dosage are to be adjusted according to the course of the surgical procedure.
Pain management in the intensive care unit: For use in pain management of ventilated patients in the intensive care unit, the dosage of fentanyl has to be adjusted individually, depending on the course of pain and on concomitant medication. Normally the initial doses are in the range of 50 to 100 micrograms i.v. (0.7-1.4 microgram/kg) but can be titrated higher if necessary.
The initial dose normally is followed by repeated injections, of up to a total of 25 to 125 micrograms fentanyl per hour (0.35-1.8 microgram/kg/h).
Dosage in Paediatric population: Children aged 12 to 17 years should follow the recommended adult dose schedule.
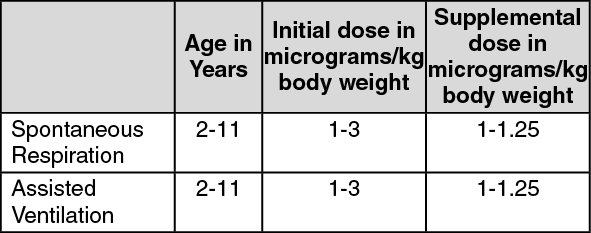
For children aged 2 to 11 years the usual dosage regimen is recommended as follows: See table.
 Click on icon to see table/diagram/image
Use in children:
Click on icon to see table/diagram/image
Use in children: Analgesia during operation, enhancement of anaesthesia with spontaneous respiration: Techniques that involve analgesia in a spontaneous breathing child should only be used as part of an anaesthetic technique, or given as part of a sedation/analgesia technique with experienced personnel in an environment that can manage sudden chest wall rigidity requiring intubation, or apnoea requiring airway support.
Dosage in elderly and weak patients: The initial dose in elderly and weak patients should be reduced. The effect of the initial dose should be taken into account for the determination of supplemental doses.
Dosage in patients with chronic opioid medication: In patients with chronic opioid medication or with a known history of opioid abuse, a higher dosage of fentanyl may be necessary.
Dosage in patients with additional diseases: In patients with one of the following diseases the intended dosage of fentanyl should be titrated very carefully: uncompensated hypothyreosis; lung diseases, especially those with reduced vital capacity; alcohol abuse; impaired hepatic function; impaired renal function.
Caution is also required if fentanyl is to be administered to patients with adrenal insufficiency, prostatic hypertrophy, porphyria and bradyarrhythmia.
In all these conditions, except alcohol abuse, the dose may have to be reduced. In alcohol abuse, the dose may have to be either reduced or increased.
In these patients a prolonged postoperative monitoring period is recommended.
ROUTE OF ADMINISTRATION: Parenteral [For IV or IM use only.]


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
